
AFib: the most commonly encountered
sustained cardiac arrhythmia.
sustained cardiac arrhythmia.
Atrial fibrillation (AF) is the most commonly encountered sustained cardiac arrhythmia (abnormal heart rhythm), and involves the two upper chambers (atria) of the heart. Its name comes from the abnormal fibrillating (i.e. quivering) of the heart muscles of the atria instead of the normal coordinated contraction.
AF prevalence increases with age with an estimated 9% prevalence in patients ages >65. It is estimated that up to 6 million people in the United States have AF; This number is expected to double by 20501-3.
AF is associated with a significant morbidity and a substantial reduction of quality of life in some patients. The consequences of atrial fibrillation range from none to debilitating, including:
- Exercise intolerance
- Congestive heart failure
- Tachycardia-induced cardiomyopathy (fast heart rate causing heart muscle damage)
- Stroke4 (clots in the brain)
AF is thought to be responsible for 15% of the strokes occurring in elderly patients1. Furthermore, AF is associated with a 50% to 100% increased risk of death4. Besides age, known risk factors for AF include hypertension, left ventricular hypertrophy (increased heart muscle thickness), diabetes, and cigarette smoking5.
AF contributes significant cost to the US healthcare system:
- $26B+ cost to US healthcare system9
- ~1M annual ER visits10
- >50% of ER visits require hospitalization11


“Atrial fibrillation begets atrial fibrillation.”
Multiple and/or prolonged episodes of AF appear to promote future episodes due to atrial remodeling, leading to forms of the disease that are harder to treat.12
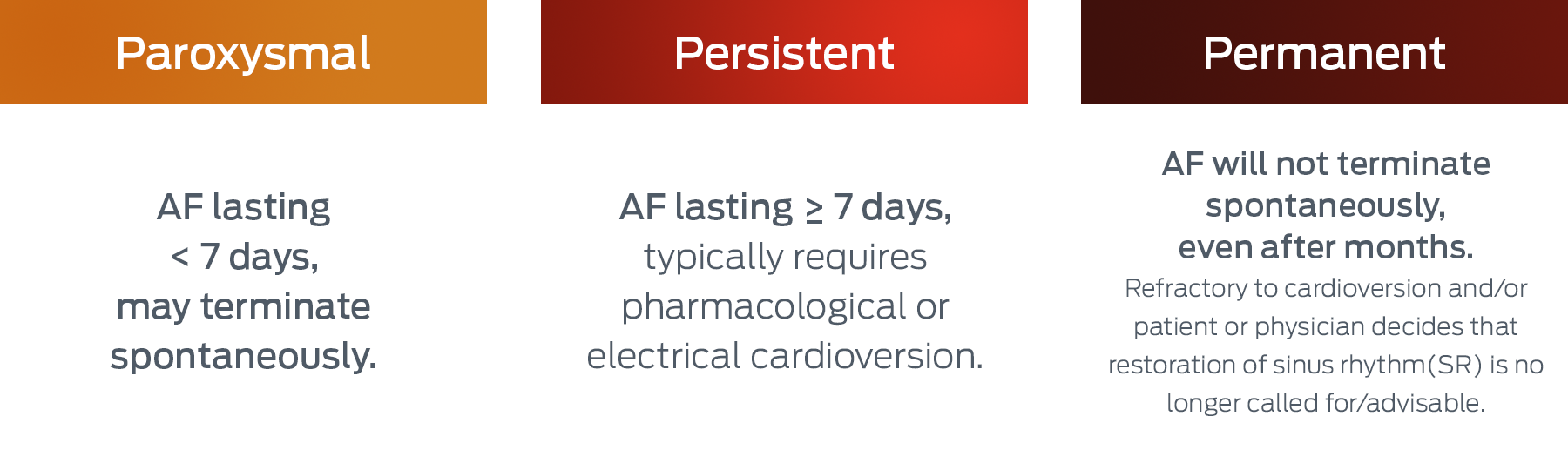
AF is a chronic, progressive condition
which is traditionally classified into three category types.6
About Paroxysmal Atrial Fibrillation (PAF)
Approximately 40% of patients with AF have paroxysmal atrial fibrillation, a type of AF where episodes terminate in less than 7 days. About 1 in 4 people with paroxysmal atrial fibrillation eventually develop the permanent form of the condition within 5 years7. Common symptoms of PAF can include:
- Racing heartbeat
- Fluttering feeling in the chest
- Chest pain or pressure
- Feeling out of breath
- Weakness or tiredness
- Dizziness and sweating
- Faintness or lightheadedness4

The Management of PAF has Three Key Objectives
-
- 1) Prevention of stroke
- 2) Relief or resolution of symptoms
- 3) Prevention of progression of AF, with its associated complications such as heart failure8
Therapeutic strategies for PAF include rate control (slowing or maintaining appropriate ventricular heart rate) and/or rhythm control (restoring or maintaining sinus rhythm). Selection of a primary therapeutic strategy is a multifactorial decision depending on the patient’s age, symptoms, frequency of episodes, comorbidities, and preference.
A recent large randomized clinical trial (EAST-AFNET 4) has shown superiority of early rhythm control over rate control alone on major cardiovascular outcomes. A number of other recent studies have provided supportive results.
Management of PAF may include both chronic and acute treatments. The goal of chronic therapy is to continuously suppress/prevent future AF episodes, or increase the time between episodes. The goal of acute therapy is to restore sinus rhythm and resolve symptoms when a patient is experiencing an episode of AF.
Today, acute treatment options for episodes of PAF include:
Rate Control Drugs
Calcium channel blockers or beta blockers taken orally or intravenously that slows the heart rate, thereby reducing symptoms.
Rhythm Control Drugs
Antiarrhythmic Drugs (AADs) taken orally or intravenously that normalize the heart rhythm (and alleviate symptoms) by its actions on ion channels in heart muscle cells. Often known as pharmacological cardioversion.
Electrical Cardioversion
A medical procedure, usually done in hospitals under general anesthesia, that normalizes heart rhythm by delivery of a quick, large electric current across the chest.
Unmet Medical Need for Acute Management of Episodes of PAF:
Today’s treatment options for episodes of PAF have several shortcomings, including:
1
Rate control drugs do not address restoration of sinus rhythm.
2
Rhythm control drugs often require several hours to take effect and/or have a poor risk-benefit profile.
3
Electrical cardioversion utilizes significant healthcare resources.
Due to these limitations, PAF patients often require hospitalization from the ER.
There is a need for a treatment option that safely and promptly restores sinus rhythm and reduces burden to the healthcare system.
1. Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 2001;285(18):2370-5.
2. January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC, Jr., et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation 2014;130(23):2071-104.
3. Chugh SS, Roth GA, Gillum RF, Mensah GA, Glob Heart. 2014 Mar;9(1):113-9
4. American Heart Association website “What are the Symptoms of Atrial Fibrillation (AFib or AF)?” www.heart .org (accessed July 2018).
5. Kannel WB, Wolf PA, Benjamin EJ, Levy D. Prevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation: population-based estimates. Am J Cardiol 1998;82(8A):2N-9N.
6. Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J 2016;37(38):2893-2962.
7. Kerr CR, Humphries KH, Talajic M, Klein GJ, Connolly SJ, Green M, Boone J, Sheldon R, Dorian P, Newman D; Am Heart J. 2005 Mar;149(3):489-96
8. Cosio FG1, Aliot E, Botto GL, Heidbüchel H, Geller CJ, Kirchhof P, De Haro JC, Frank R, Villacastin JP, Vijgen J, Crijns H, Europace. 2008 Jan;10(1):21-7. Epub 2007 Dec 17
9. Kim et al, Circulation 2011
10. Rozen, Ruskin et al. J Am Heart Assoc. 2018
11. Go et al, JAMA 2001
12. Nattel S, Guasch E, Savelieva I, et al. Early management of atrial fibrillation to prevent cardiovascular complications. Eur Heart J. 2014;35:1448-1456.